Few things calm post-operative anxiety like knowing what is supposed to happen on each day. Families often arrive at their first consultation with a clear picture of why their child needs the Nuss procedure to correct pectus excavatum, but only a fuzzy idea of what comes next. This guide walks through the recovery week by week, from the first hours after surgery through the slow return to full sport. Knowing what Nuss procedure recovery looks like in advance is one of the best ways to ease the uncertainty.
Every patient’s path is slightly different. Younger patients tend to bounce back faster. More complex chests, longer surgeries, or stiffer bars stretch the timeline. The milestones below are the typical shape rather than a strict schedule, and your surgical team will tailor the plan to your case. With that caveat in mind, here is what most families can expect.
Before you go in: what Nuss procedure recovery actually requires
Recovery from a Nuss procedure asks for three things: pain management, restricted movement, and patience. None of them are dramatic in isolation. Together, they ask families to slow down for a few weeks and to accept that healing happens at its own pace.
Most patients are in hospital for four to six days, then at home for two to three weeks of structured rest, then in a gradual return-to-activity phase that runs for two to three more months. By the end of the third month, ordinary life is fully restored, even if certain sports are still off-limits.
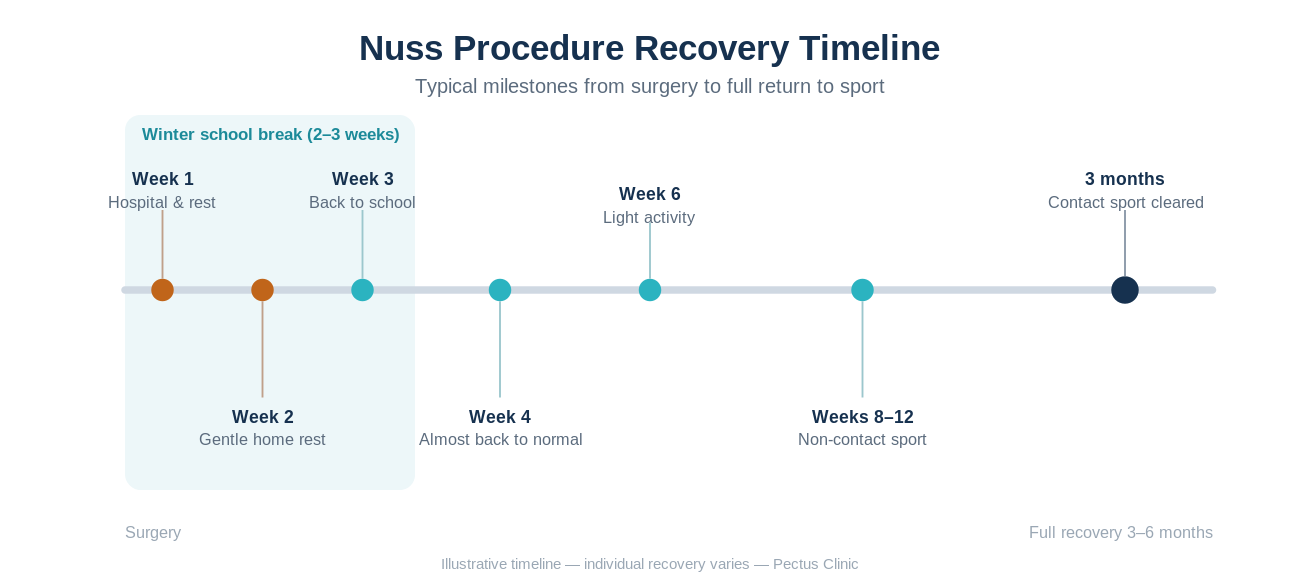
Week 1: hospital, the first walk, and the journey home
The first forty-eight hours focus on pain. Most patients have an epidural delivering continuous analgesia, supplemented by anti-inflammatory and muscle-relaxant medication. Nurses encourage sitting up at the edge of the bed by day one, and the first short walk usually happens on day two. Walking is a real turning point. It moves fluid, supports lung expansion, and reassures the patient that the body still works.
By days three and four, the epidural is replaced with oral pain medication, and the focus shifts to chest physiotherapy, breathing exercises, and walking laps of the ward. Discharge typically happens between day four and day six, once the patient can walk comfortably, eat normally, and manage pain on tablets alone.
The drive home is often the most uncomfortable part of week one. A pillow held against the chest helps with bumps in the road. The first night in a familiar bed is, paradoxically, where many patients sleep best.
Week 2: the quietest week
Week two is the quietest week of the whole recovery. The patient stays home, sleeps with the upper body propped on pillows, walks slowly around the house and garden, and avoids any bending, twisting, or lifting. Activities like reading, screen time, sitting at a desk for short periods, and gentle conversation with visiting friends are all encouraged.
Pain medication is still on a regular schedule, but doses tend to drop steadily by the end of the week. Most patients can manage on basic analgesia by day ten to twelve.
A common surprise: tiredness is more present than pain. The body is spending real energy on healing, and naps are normal.
Weeks 3 and 4: returning to the world
By the start of week three, most patients are walking comfortably outside, sitting upright for longer, and beginning to look beyond the recovery cocoon. School returns in stages for younger patients, often a half day on a Monday, a full day by Wednesday, and a normal week by week four. Heavy backpacks are out. A wheeled bag or a split set of textbooks handles the load.
Movement restrictions are still in force. Bending, twisting, lifting more than two or three kilograms, and any contact are off limits. The bar inside the chest is still settling into position, and protecting it for these weeks is the single most important thing the patient can do.
By week four, most patients describe themselves as feeling normal in everyday life, even if exercise is still some distance away.
Weeks 5 and 6: back at school, ready for light movement
Week five marks the start of light, structured activity. Stationary cycling at low resistance, gentle walking outdoors, and very light yoga focused on breath rather than postures are all reasonable. Swimming returns in week six, as long as it is calm lap swimming rather than competitive training.
PE remains off the calendar. Most schools accept a one-page letter from the surgical team explaining that the patient sits out for the full first term back.
Weeks 7 to 12: building toward sport
Weeks seven through twelve are the gradual ramp-up phase. Jogging is reintroduced. Non-contact training drills begin. Cricket batting, golf, dance practice, and gentle resistance work all come back online during this window, with the surgeon’s clearance.
Contact sport waits until the end of week twelve at the earliest. Rugby, hockey, water polo, martial arts, and gymnastics involving falls or impact stay paused. The bar is well settled by this point, but a direct blow is still capable of shifting it, and the cost of a complication outweighs a few weeks of patience.
Month four to month six: almost back to normal
Most patients reach month four describing themselves as fully recovered. The bar is no longer felt during ordinary movement, sleep is normal again, and confidence in the chest returns. Contact sport is generally cleared between months four and six, depending on the patient and the sport.
Living with the bar: the longer view
The Nuss bar typically stays in place for two to three years before a short outpatient procedure to remove it. Day-to-day life with the bar is unremarkable for most people. Airport metal detectors will notice it, so a letter from the surgeon for travel is useful. MRI scans are still possible with modern bars but require coordination. Regular activity, including competitive sport, is fine once the recovery phase is complete.
When to call your surgeon
Most recoveries are uneventful. Still, certain signals warrant a phone call:
- Rising fever after week one.
- Increasing rather than decreasing pain.
- Redness or discharge at the incision sites.
- Sudden shortness of breath that feels different from the usual post-operative tightness.
- Any sense that something has shifted inside the chest after a fall or sudden movement.
None of these are common. All of them are worth a quick check.
A note for adults
Adult Nuss procedure recovery follows the same broad shape but tends to feel a bit slower in the early phase. Pain is often more pronounced because the adult chest is stiffer, and the return to desk work usually happens around week three rather than week two. Return to gym and contact sport tracks the same three-month minimum.
Related reading: Planning pectus surgery around the South African school calendar and pectus excavatum and asthma-like symptoms in cooler weather.
If you are preparing for a Nuss procedure with Dr. Schewitz, or considering one, the team will walk through this timeline in detail at your consultation. Every patient’s recovery is shaped around their age, fitness, sport, school, and family circumstances. Book an in-person or online consultation to start mapping your own plan.