As the South African autumn tips toward winter, GP waiting rooms fill up with patients, and parents of patients, describing the same cluster of symptoms: shortness of breath on a morning walk, a tight chest after netball practice, a cough that lingers after the school run. For most, the answer is a straightforward respiratory infection or a flare-up of asthma. But for a smaller group, the real culprit has been sitting in plain sight all along: pectus excavatum, the sunken-chest deformity that subtly reshapes how the lungs and heart share space inside the ribcage.
If you or your child has been told “it’s just asthma” but the inhaler only helps a little, or the symptoms keep returning each cold season, it’s worth understanding how pectus excavatum and asthma can look almost identical, and why winter often pushes a quietly-tolerated chest wall difference into something that can no longer be ignored.
How pectus excavatum affects breathing in the first place
Pectus excavatum is a congenital difference in which the breastbone (sternum) and the cartilage connecting it to the ribs grow inward, creating a visible hollow in the centre of the chest. In mild cases the appearance is mostly cosmetic. In moderate to severe cases, the inward curve reduces the space the lungs have to expand and can press on the heart, nudging it to the left.
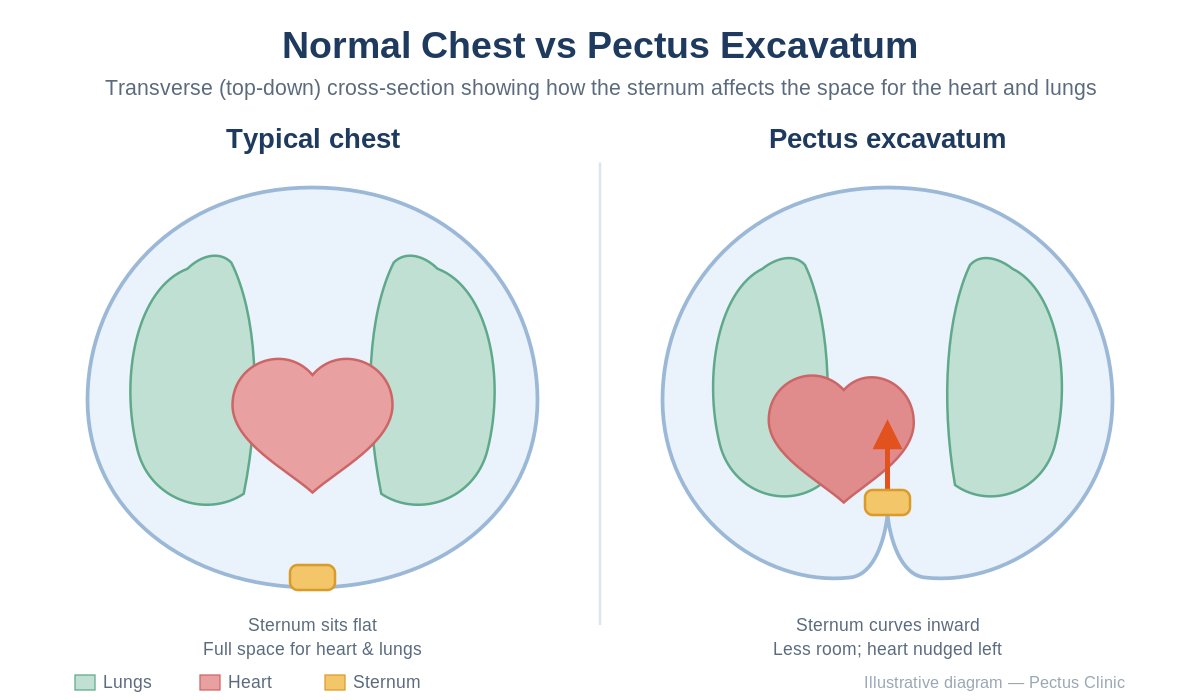
The functional result is a chest that works a little harder for the same amount of air. At rest, most people compensate without noticing. But during exercise, illness, or cold weather, when the airways naturally constrict and breathing demand rises, that small mechanical disadvantage can tip into real symptoms: breathlessness, chest tightness, early fatigue during sport, and a wheeze or cough that mimics asthma.
Why cooler weather makes pectus symptoms louder
South African winters are milder than European ones, but the temperature swing between a 28°C February afternoon and a 6°C July morning is enough to provoke measurable changes in the airways. Three things happen at once:
Cold air causes the small airways in the lungs to narrow reflexively, raising the work of breathing for everyone, but more so for a chest that is already mechanically compressed. Respiratory viruses peak between April and August, adding inflammation on top of an already constrained system. And physical activity in cold, dry air dries out the airway lining, triggering the same cough-and-wheeze pattern clinicians associate with exercise-induced asthma.
For a person with pectus excavatum, these seasonal factors stack on top of an anatomical baseline. The symptoms that were a quiet annoyance in summer become the reason parents book a GP appointment in May.
Pectus excavatum vs asthma: how to tell them apart
There’s a reason misdiagnosis is so common. Both conditions can produce shortness of breath, chest tightness, reduced exercise tolerance, and a cough. But the patterns are different if you know what to look for.

Asthma is driven by airway inflammation. It typically responds well to a bronchodilator inhaler within minutes, flares around specific triggers (dust, pollen, pets, viruses), often runs in families alongside eczema or hay fever, and shows characteristic patterns on spirometry and peak-flow testing.
Pectus-related breathing difficulty is driven by mechanical restriction. It tends to be more constant than episodic, often worsens gradually through adolescence as the chest grows, may only partially improve with an inhaler, and is accompanied by a visible or palpable dip in the chest wall. Parents will sometimes describe their teen as “always been a bit winded” rather than pinpointing a specific onset.
The giveaway is often in the exam: a patient whose inhaler keeps being escalated without full relief, or whose lung function tests look less impaired than their symptoms suggest, deserves a careful look at the chest wall itself.
Why pectus excavatum gets missed, even by good doctors
Pectus excavatum is not rare, affecting roughly 1 in every 300 to 400 children, with boys more commonly affected than girls. But it’s easy to overlook for three reasons.
First, it is often hidden. Teenagers are self-conscious about their chests and may avoid changing in front of parents, meaning the hollow is noticed late. Second, symptoms often only emerge during the growth spurt of puberty, at precisely the age when asthma, allergies, and general deconditioning are common alternative explanations. Third, GPs understandably reach for the most statistically likely diagnosis first, and inhalers are a reasonable early step.
None of this is a failure of care. It simply means that when the inhalers don’t resolve the story, a specialist opinion is the next logical step, rather than another dose adjustment.
When to seek a specialist assessment
Consider a referral to a pectus specialist if any of the following apply:
- A visible dip in the centre of the chest, whether long-standing or recently noticed.
- Shortness of breath or chest tightness that returns every cold season despite asthma treatment.
- Exercise intolerance that doesn’t match the person’s fitness level.
- Fatigue, palpitations, or the sense that the heart “feels off” after exertion.
- A teenager who has quietly stopped playing sport or swimming because of how their chest looks or feels.
Adults are often surprised to learn that pectus excavatum can be corrected well into their thirties and forties. It is not a condition exclusive to children, and symptoms that were tolerable for years can become meaningful as cardiovascular demand increases with age.
What a specialist consultation involves
At Pectus Clinic, assessment typically includes a physical examination, imaging to measure the severity of the deformity (using the Haller Index, a ratio of chest width to depth), and cardiac and pulmonary function testing to quantify whether the chest shape is affecting how the heart and lungs work. Only after that is a treatment path discussed, which may range from external bracing and the vacuum bell for milder cases, to the minimally-invasive Nuss procedure or the Reverse Nuss for more complex presentations.
Online consultations are available for patients outside Johannesburg, Cape Town, and Durban, which makes the first step genuinely low-friction.
The takeaway
If breathing symptoms worsen every autumn and winter, and an inhaler is only doing part of the job, it’s worth asking a second question: is this really asthma, or is the chest wall itself part of the picture? Pectus excavatum is treatable, often elegantly so, and identifying it changes what good care looks like. The earlier the conversation starts, the more options remain on the table.
Related reading: planning pectus surgery around the South African school calendar and the week-by-week Nuss recovery guide.
Ready to find out whether pectus excavatum is contributing to your symptoms? Book a consultation with Dr. Schewitz or request an online assessment. It’s your first step toward breathing more easily through next winter.